


Clinical endocrinology
BACKGROUND: The prevalence of SHPT depends on control strategy and target level of PTH. There is insufficient data for a justified choice of goals and strategy for the SHPT correction.
AIM: A retrospective, multicenter, cohort study was conducted to assess the ethelcalcetide efficacy after six months in real world practice. The study sought to identify whether MBD-CKD characteristics are predictive of achieving the goals.
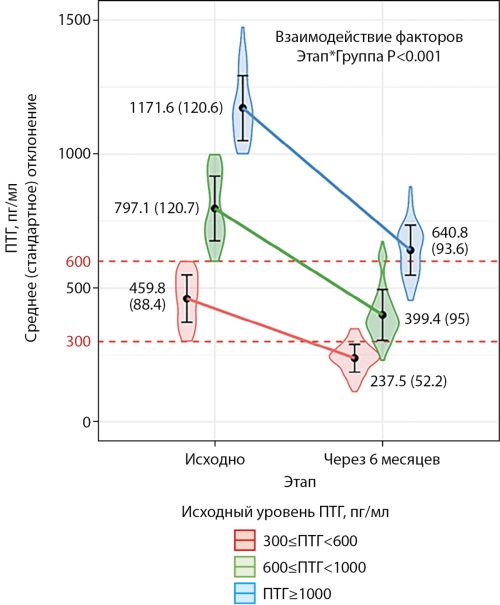
MATERIALS AND METHODS: A study included 302 patients in 20 dialysis units in St. Petersburg. The primary endpoint was the proportion of patients who reached the target of PTH (300–599 pg/ml). The secondary endpoint was an absolute and relative decrease in PTH. The results were compared in subgroups with PTH (<600, 600–1000, ≥1000 pg/ml) and with and without signs of parathyroid authonomy.
RESULTS: In patients aged 56 (12) years (men — 61%) with a dialysis duration of 36 (Q1-Q3 23-55) months with baseline PTH level of 729 (548–957) pg/ml and with calcemia and phosphatemia 2.35 (0.25) and 1.97 (0.47) mM/L, the proportion of success was 49.7%. It is more expected for the PTH of 600–1000 pg/ml compared with PTH>1000 pg/ml: 79% vs. 36%, p<0.001. In presence of signs of parathyroid authonomy, 48% reached the target range vs. 86% in its absence (p<0.001) in subgroup with PTH of 600–1000 pg/ml. For patients with PTH above 1000 pg/ml, the proportion was 25% vs. 58% (p=0.016). The signs of parathyroid authonomy was the most significant independent risk for target achieving (OR=0.3 [95% CI 0.13; 0.68], p=0.004)
CONCLUSION: When transferring patients from cinacalcet to etelcalcetide, no new side effects or drug intolerance were noted. In moderate SHPT (PTH 600–1000 pg/ml) it is possible to achieve the target in most patients, but with higher level, the result worsened. The signs of parathyroid authonomy predicts the insufficient effect better than high baseline PTH level.
BACKGROUND: Thyroid hormone replacement therapy results remain unsatisfactory in 30-50% of cases. To differentiate between true levothyroxine sodium malabsorption and pseudomalabsorption due to poor compliance, several absorption assessment tests with different evaluation criteria are proposed.
AIM: To determine the criteria for normal absorption of levothyroxine sodium when performing an oral test with a single bolus dose of 600 mсg.
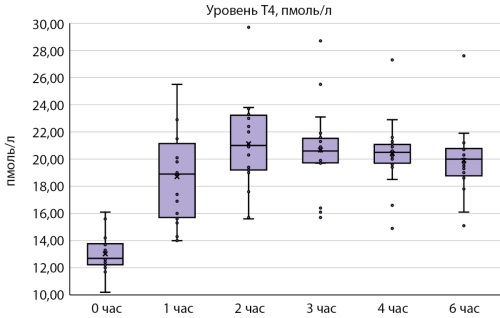
MATERIALS AND METHODS: The study involved 20 healthy volunteers of both sexes, aged 18 to 35 years, with normal body weight. The bolus dose of levothyroxine sodium was 600 mсg. Blood samples for determination of free thyroxine (fT4) concentration in serum were taken on an empty stomach, 1 hour, 2, 3, 4, 6 hours after taking the drug.
RESULTS: After taking levothyroxine sodium at a dose of 600 mcg, the maximum level of free T4 was observed after 2 hours — 21,00 pmol/l [19,20; 23,16]. The minimum increase in the concentration of free T4 2 hours after taking levothyroxine sodium at a dose of 600 mcg was — 18,0%, the maximum — 91,1%.
CONCLUSION: To assess the absorption of levothyroxine sodium, a single oral dose of 600 mcg of levothyroxine sodium is recommended. Absorption of levothyroxine sodium can be considered normal if the increase in free T4 concentration 2, 3, or 4 hours after the bolus dose is at least 18%.

This clinical case demonstrates difficulties in managing patients with newly diagnosed hypercalcemia. Depending on the involvement of parathyroid hormone (PTG) in the mechanisms of hypercalcemia the latter is divided into parathyroid hormone-dependent (PTH-dependent) and parathyroid hormone-independent (PTH-independent). In this clinical case an analysis of clinical, laboratory and instrumental data revealed a rare combination of PTH-dependent and PTH-independent hypercalcemia. A 74-year-old patient was diagnosed with primary hyperparathyroidism (PHPT) which was the cause of severe hypercalcemia. Persistence of hypercalcemia after surgical treatment and normalisation of PTH levels required further diagnostic search and exclusion of other causes of hypercalcemia. As a result, sarcoidosis with lesions of the mediastinal and cervical lymph nodes was revealed. Methylprednisolone was administered in the treatment regimen, which gradually normalised serum calcium levels.

Thyroid eye disease (TED) is an autoimmune pathology of the orbital tissues associated with autoimmune thyroid disease, most commonly occurring with Graves’ disease. The clinical presentation of TED is extremely diverse, ranging from mild orbital involvement to potentially vision-threatening optical neuropathy. Early diagnosis of the active phase of TED is crucial, as immunosuppressive therapy is effective only during this phase, while treatment for patients in the inactive phase consists only of rehabilitative surgery. High-dose intravenous glucocorticoids are the first-line treatment for patients with moderate to severe active TED. Glucocorticoids are widely used due to their anti-inflammatory and immunosuppressive properties, but about 20–30% of patients remain resistant to glucocorticoid treatment. One promising direction in the treatment of glucocorticoid-resistant TED is the use of monoclonal antibodies targeting specific antigen epitopes. We present a clinical case of tocilizumab treatment in severe glucocorticoid-resistant TED complicated by optic neuropathy.
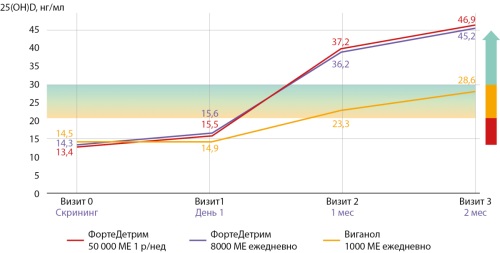
This article presents an overview of current research on determining target blood levels of vitamin D. It examines the biochemical and metabolic properties of vitamin D, as well as the challenges of standardizing 25(OH)D measurements and the variability of threshold values across populations. It discusses ambiguities in scientific data and the need to consider individual factors when interpreting vitamin D levels. This review is unique in its comprehensive approach to analyzing the effects of vitamin D not only on bone health but also on immune and metabolic functions, which broadens ever evolving understanding of the clinical significance of vitamin D. This work emphasizes the importance of personalized recommendations for vitamin D dosing and prescription based on current clinical data and scientific standards. Performed analysis highlights the need for personalized vitamin D supplementation to reach and maintain blood levels between 30 and 60 ng/mL, noting that higher levels might be necessary for people with genetic or acquired resistance. These insights substantiate the development of evidence-based, personalized clinical strategies for the prevention and treatment of vitamin D deficiency-related disorders. The synthesized data offer significant implications for advancing research and clinical practice in endocrinology, obstetrics, dermatology, neurology and immunology.
Experimental endocrinology
BACKGROUND. Recurrent hypoglycemia occurs during insulin therapy in patients with diabetes mellitus and is a significant cause of brain dysfunction in these patients. The functioning of the hematocerebrospinal fluid barrier and the production of cerebrospinal fluid (CSF) are of great importance in ensuring brain activity. The main volume of CSF is formed by the choroid plexus of the lateral ventricles (LV) of the brain and the glymphatic system of the brain. The role of the choroid plexus in the development of brain dysfunction in hypoglycemia has not been sufficiently studied.
OBJECTIVE. The aim of this work was to determine the structure of the choroid plexuses of the lateral ventricles of the brain during recurrent hypoglycemia.
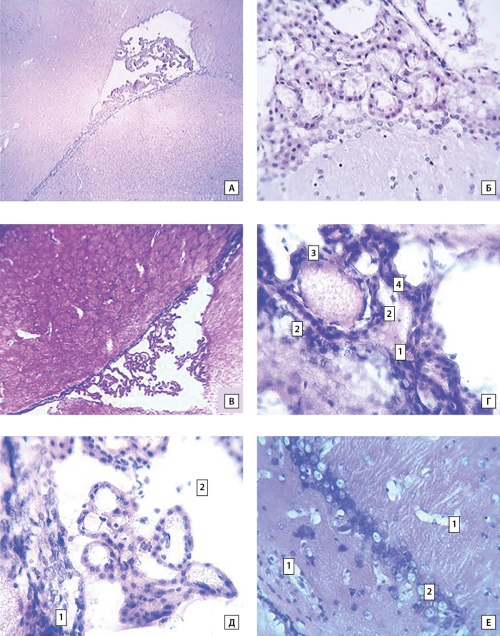
MATERIALS AND METHODS. The object of the study were rats that had undergone 9 hypoglycemic states after insulin administration (with an interval of 3 days, the blood glucose level of 1.4–1.8 mmol/L) and intact animals. The volume of the LV and volume fractions of the choroid plexuses in the LV were estimated: the relative volume and total fraction of vessels, fractions of cells and connective tissue. Morphological changes in the epithelium of the choroid plexus and nervous tissue of the periventricular spaces were also recorded.
RESULTS. In animals that had undergone a series of hypoglycemias, the maximum cross-sectional area of the LV, the relative volume of the choroid plexuses of the LV and the volume fraction of vessels per volume of the choroid plexus of the LV increase. The volume fraction of cells per volume of the choroid plexus of the ventricles decreases in rats with recurrent hypoglycemia. Morphological examination of these animals reveals dystrophic changes in the epithelial cells of the choroid plexus and zones of dystrophic changes in the brain tissue surrounding the ventricles.
CONCLUSION. Thus, recurrent hypoglycemia leads to an increase in the maximum cross-sectional area of the LV and the relative volume of the choroid plexuses, as well as dystrophic changes in the epithelial cells of the choroid plexuses and neurons of the periventricular spaces. Since hypoglycemia is repeatedly observed during the treatment of patients with diabetes mellitus, the identified changes may cause cognitive impairment and the development of dementia in these patients.
Oncoendocrinology
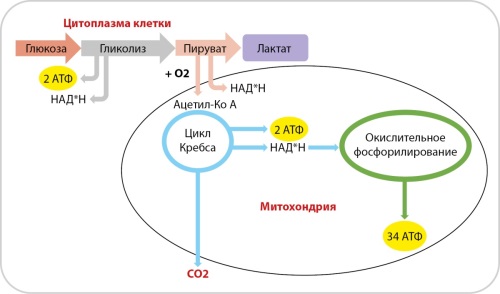
The basis of the vital activity of each cell of the body is energy metabolism, necessary for the implementation of physiological needs in norm and pathology. The most important pathways for the synthesis of adenosine triphosphate are glycolysis, the tricarboxylic acid cycle and oxidative phosphorylation. Glucose, free fatty acids and amino acids can be used as a substrate for obtaining energy. As the disease develops, reprogramming occurs in cells with the ability to switch between energy pathways and the choice of its sources, forming a specific metabolic phenotype that ensures cell survival and the formation of clinical characteristics of the disease. The availability of information on pathophysiological changes at the level of cell metabolism is of scientific and practical interest in relation to the development of methods for accurate diagnosis and the choice of personalized tactics in each specific case. This review describes the characteristics of energy metabolism in normal and tumor cells. It also provides information on modern methods for assessing energy metabolism in the body.
Carbohidrates metabolism disturbancies
BACKGROUND. Currently, diabetes mellitus is studied as an urgent social problem. This is due to the fact that the number of identified cases is constantly growing, the course of the disease often becomes chronic, various complications develop, which lead to a deterioration in the quality of life and a reduction in its duration. At the moment, there are many blood glucose monitoring systems that differ in measurement accuracy, which is important not only for daily monitoring, emergency measurement when health deteriorates, but also for selecting an adequate dose of insulin. With the advent of a new product on the consumer market, in particular the Gmate LIFE blood glucose monitoring system, many questions arise — is the device as reliable and accurate as the manufacturer claims?
AIM. To evaluate whether the measurement accuracy of the domestic Gmate LIFE blood glucose monitoring system meets the requirements of GOST R ISO 15197-2015 «In vitro diagnostic test systems. Requirements for blood glucose monitoring systems for self-testing in managing diabetes mellitus» (identical to International ISO 15197:2013).
MATERIALS AND METHODS. The design of experiments to study the measurement accuracy of the Gmate LIFE glucose monitoring system was guided by the requirements of GOST R ISO 15197-2015. The accuracy of the system was studied on capillary blood samples. Capillary blood samples were taken from healthy individuals, as well as from outpatients with hypoglycemic and hyperglycemic conditions in the endocrinology department of the Irkutsk Regional State Autonomous Healthcare Institution «Irkutsk City Clinical Hospital No. 10». The studies were conducted from 05.03.2025 to 06.03.2025 in the endocrinology department of the Irkutsk Regional State Autonomous Healthcare Institution «Irkutsk City Clinical Hospital No. 10».
RESULTS. To evaluate the accuracy of the system, 600 capillary blood samples were tested, obtained from volunteers — mainly outpatients with diabetes mellitus or inpatients. The results met the minimum accuracy criteria of the GOST R ISO 15197-2015 standard.
CONCLUSION. The result of tests for measuring blood glucose levels depends on the technology and quality of the glucometer and test strips. The system must meet the minimum requirements of the GOST R ISO 15197-2015 standard. Testing of the Gmate LIFE system showed that the results of accuracy of the Gmate LIFE glucose monitoring system fully comply with the standard, and according to the system accuracy criterion, they show a result better than specified in the requirements.
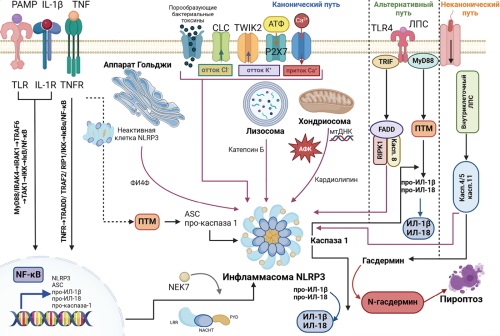
According to recent studies, chronic systemic inflammation mediated by activation of the inflammasome NOD-like receptor protein 3 (NLRP3) is a key factor in the pathophysiology of type 2 diabetes mellitus (DM). The main features of the activation of signalling cascades and regulatory mechanisms of the NLRP3 inflammasome in type 2 DM are related to the fact that glucose, saturated fatty acids, lipotoxic ceramides, oxidised LDL and cholesterol act as the main molecular patterns associated with damage, activating the inflammasome and triggering a cascade of signalling mechanisms leading to the production of IL-1β and pro-inflammatory cytokines. A number of antidiabetic drugs not only effectively control glucose levels, but also correct immunometabolic disorders associated with NLRP3 inflammasome activation. Given the role of interleukin-1β (IL-1β) in the inflammation associated with type 2 DM, anti-IL-1 therapies such as anakinra, canakinumab and gevokizumab are being investigated in both experimental models of DM and clinical trials. However, the use of this group is limited by the increased risk of infection. Among the inhibitors of NLRP3 inflammasome activation, MCC950, OLT1177, CY-09 are the most studied, but none of the compounds in this group are currently used in clinical practice. The aim of this review is to assess the role of the NLRP3 inflammasome in the pathogenesis of type 2 diabetes, as well as the potential of inflammasome pathway inhibitors as promising therapeutic agents.
Pediatric Endocrinology

BACKGROUND: Thyroid nodules in children are relatively rare; the risk of malignancy is considerably higher compared to adults. The optimal extent of surgery, the indications for radioactive iodine therapy (RAI), and the role of molecular genetic testing in children with thyroid carcinoma remain a matter of debate.
AIM: To investigate the clinical course of differentiated thyroid carcinoma (DTC) in children, as well as the outcomes of surgical and combined treatment based on ten years clinical experience at the Endocrinology Research Centre.
MATERIALS AND METHODS: This retrospective single-center study included 980 pediatric and adolescent patients who underwent surgery for thyroid nodules between 2015 and 2024. The diagnostic protocol comprised history taking, physical examination, thyroid ultrasound, fine-needle aspiration biopsy, and postoperative histopathological evaluation. Molecular genetic testing was performed in children with a family history or suspected syndromic forms of thyroid carcinoma. The median follow-up duration for patients with DTC was 12 months [1.0; 36.0].
RESULTS: Malignant thyroid tumors were identified in 506 patients (51.6%), the majority of them — differentiated thyroid carcinoma (DTC) (n=472). The most common histological type was papillary thyroid carcinoma (n=448; 88,5%). Metastatic involvement of regional lymph nodes was present in 21% of children. Adjuvant RAI was performed in 48.5% of patients; distant metastases to the lungs were detected in 5.7% of cases. Recurrences were registered in 5.1% of children; in 16.5% of children the disease persisted after primary treatment in the form of biochemical and/or structural persistence. MGI was performed in 66 children; pathogenic variants were detected in 53.1%, most frequently in the DICER1, PTEN, and APC genes.
CONCLUSION: Differentiated thyroid carcinoma in children is characterized by a number of clinical and molecular genetic features, which determines the need for a specialized multidisciplinary approach to their management. The high risk of malignancy in nodules, frequent regional dissemination and peculiarities of the molecular profile argue for the necessity of early diagnosis, integration of molecular testing and personalized choice of the volume of surgical intervention in the conditions of specialized centers.
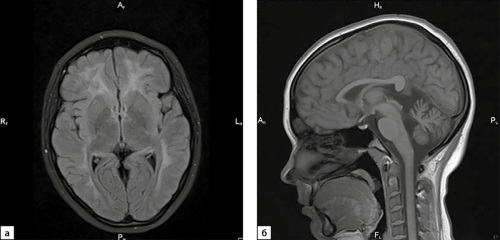
Congenital hypogonadotropic hypogonadism (СНH) is a group of diseases caused by impaired synthesis or secretion of gonadotropin-releasing hormone (GnRH) and gonadotropin hormones. At present, more than twenty genes involved in the development of СНН have been described. In the structure of HGH, the most common forms of the disease are caused by pathogenic variants in genes involved in the ontogenesis, migration and survival of GnRH neurons, whereas pathology of genes involved in the action/transmission of GnRH signals in normally developed GnRH neurons is less common. This article describes a rare variant of СНН as a result of pathogenic variants in the POLR3B gene, occurring in 1.1% of cases of СНН, which is a component of hypomyelinating leukodystrophy 4H and includes hypomyelination, CHН, hypodontia. Identification of the genetic nature of the disease in this patient made it possible not only to establish the cause of CНН, but also to diagnose comorbid conditions.
Lipoid adrenal hyperplasia (LAH) is a rare severe form of congenital adrenal hyperplasia, which is caused by mutations in the STAR gene (8p11.2), encoding the transport protein StAR. The defect of the StAR protein leads to a total disruption of adrenal and gonadal steroidogenesis. The division into the classic form of the disease, in which all steroidogenesis is disrupted, and the non-classic, in which only adrenal steroidogenesis is usually disrupted, is a generally accepted classification of LAH. We report two cases of patients with clinical and laboratory data indicating a non-classic LAH. Both patients with 46,XY karyotype presented late (at 5 and 3 years) manifestation of clinical symptoms and had normal male external genitalia. Homozygous mutation p.R188C in one patient and compound heterozygous mutations p.R188C and p.R272H in the other were identified by molecular genetic assay. STAR genetic testing allowed to diagnose non-classic LAH in differential diagnosis of hypocorticism.
Reproductive Endocrinology
Menopausal symptoms can disrupt the lives of women at the peak of their careers and family life. Currently, the most effective treatment for these symptoms is menopausal hormone therapy (MHT). The presence of cardiovascular and metabolic diseases does not preclude the use of MHT to relieve menopausal symptoms and improve quality of life. However, physicians’ concerns about causing more harm than good often hinder the use of this type of hormone therapy. Caution is especially important when it comes to women with comorbidities. Moreover, it should be acknowledged that high-quality studies on the safety of MHT for major chronic noncommunicable diseases and common comorbid conditions are insufficient. This consensus document analyzes all currently available data from clinical trials of various designs and develops a set of eligibility criteria for prescribing MHT to women with comorbid cardiovascular and metabolic diseases. Based on this document, physicians of various specialties who consult with women in menopause will receive an accessible algorithm that will allow them to avoid potentially dangerous situations and appropriately prescribe HRT in clinical practice.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0).
ISSN 2308-1430 (Online)





































